Results 71 to 80 of 80
-
03-23-2011 #71Rookie Poster

- Join Date
- Jan 2009
- Location
- in the kitchen
- Posts
- 91
 Re: tgirl lovers/admirers are gay yes??
Why exactly is gay sex better than sex with girls?
Re: tgirl lovers/admirers are gay yes??
Why exactly is gay sex better than sex with girls? Originally Posted by maleforts
Originally Posted by maleforts

-
03-23-2011 #72Senior Member Veteran Poster
- Join Date
- Sep 2010
- Location
- Baltimore, Maryland
- Posts
- 229
 Re: tgirl lovers/admirers are gay yes??
Re: tgirl lovers/admirers are gay yes??

-
03-23-2011 #73Junior Poster
- Join Date
- Jan 2008
- Location
- ohio
- Posts
- 251
Re: tgirl lovers/admirers are gay yes??
Maleforts I dont think you should try to put everyone in a certain category so you can compartmentalize the way you judge and feel about yourself. In saying im this so everyone who shares this and this with me are that. It really doesnt work like that. People are all different. Dont judge or label anyone other then yourself. Why is it so important to come up with a title for every person on the planet? The answer it isnt. Just be yourself. and to thine own self be true
-
03-23-2011 #74Platinum Poster

- Join Date
- Mar 2006
- Location
- hollywood,calif
- Posts
- 7,071
 Re: tgirl lovers/admirers are gay yes??
Re: tgirl lovers/admirers are gay yes??
what are hermaphrodites?
are hermaphrodites intersexed?
http://jl10ll.wordpress.com/2010/11/...ent-surgeries/
http://www.google.com/images?hl=en&s...w=1345&bih=562
hermaphrodites - Google Search


Originally Posted by maleforts
-
03-23-2011 #75Platinum Poster
- Join Date
- Mar 2006
- Location
- hollywood,calif
- Posts
- 7,071
Re: tgirl lovers/admirers are gay yes??
Born a Boy Raised a Girl – The John/Joan/David Reimer Case and Sex Reassignment Surgery
Posted on November 5, 2010 by teacher
David Reimer - Wikipedia, the free encyclopedia, well known in medical and psychiatric circles specializing in gender Sex assignment - Wikipedia, the free encyclopedia, served as a ground-breaking study in regard to sexual orientation and sexual identity.
 Reimer was born a boy with an identical (monozygotic) male twin. (Yes it is possible for a boy and a girl to be nearly “identical” and to have begun as monozygotic twins in the womb … if you’re interested read my blog Seeing (almost) Double).
Reimer was born a boy with an identical (monozygotic) male twin. (Yes it is possible for a boy and a girl to be nearly “identical” and to have begun as monozygotic twins in the womb … if you’re interested read my blog Seeing (almost) Double).
 In 1966, a botched electrical Circumcision - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Circumcision_central_Asia2.jpg" class="image">
In 1966, a botched electrical Circumcision - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Circumcision_central_Asia2.jpg" class="image"> left David Reimer (then named Bruce) without a penis. A malfunction in the doctor’s equipment (electro-cautery needle) caused the needle to burn Reimer’s penis from tip to base. The Reimers were left with a dilemma: a son with no penis. They visited several medical experts who assured them that penile reconstruction would prove worthless. The Reimers were at a loss as to how to help David. One afternoon when the Reimers saw Dr. John Money, a so-called expert in sex reassignment, on television they contacted him and brought their son to see him. It would prove to be a tragic decision.
left David Reimer (then named Bruce) without a penis. A malfunction in the doctor’s equipment (electro-cautery needle) caused the needle to burn Reimer’s penis from tip to base. The Reimers were left with a dilemma: a son with no penis. They visited several medical experts who assured them that penile reconstruction would prove worthless. The Reimers were at a loss as to how to help David. One afternoon when the Reimers saw Dr. John Money, a so-called expert in sex reassignment, on television they contacted him and brought their son to see him. It would prove to be a tragic decision.
Money met with ”Brenda” once a year throughout the following years to report on her progress. In spite of growing evidence that Brenda was not adjusting well to her gender reassignment, Money published papers to the contrary. In psychiatric circles to protect Reimer’s identity Money referred to “Brenda” as John/Joan . Money’s experiment became well-known in psychiatric communities worldwide and partly as a result of Money’s publications, a number of infants born with ambiguous genitalia underwent gender reassignment. However many psychologists were unconvinced about the John/Joan experiment. One of these was academic sexologist Milton Diamond - Wikipedia, the free encyclopedia, who, in a bold move against Money reported to the psychiatric community that Reimer never identified as female, and that he began living as a male from the age of 15.
 Sexual reassignment in the Reimer case is not a gender identity disorder. He was born male unlike than intersex (Hermaphrodite - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Text_document_with_red_question_mark.svg" class="image">
Sexual reassignment in the Reimer case is not a gender identity disorder. He was born male unlike than intersex (Hermaphrodite - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Text_document_with_red_question_mark.svg" class="image"> ) individuals. Intersex - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Hermaphroditus,_from_a_Pompeiian_fresco,_c.18 00_(coloured_engraving)_by_French_School,_(19th_ce ntury).jpg" class="image">
) individuals. Intersex - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Hermaphroditus,_from_a_Pompeiian_fresco,_c.18 00_(coloured_engraving)_by_French_School,_(19th_ce ntury).jpg" class="image"> is a term that usually defines discordance of the biological aspects of sexual gender. Traits related to the genitalia, such as internal organs, Gonad - Wikipedia, the free encyclopedia tissue, or Chromosome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Chromosome.svg" class="image">
is a term that usually defines discordance of the biological aspects of sexual gender. Traits related to the genitalia, such as internal organs, Gonad - Wikipedia, the free encyclopedia tissue, or Chromosome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Chromosome.svg" class="image">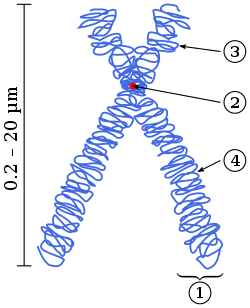 that are more typical of the other sex, or incompletely Sexual differentiation - Wikipedia, the free encyclopedia define the intersex individual.Sub-types of hermaphroditism include:
that are more typical of the other sex, or incompletely Sexual differentiation - Wikipedia, the free encyclopedia define the intersex individual.Sub-types of hermaphroditism include:
- Pseudohermaphroditism Typically a female has a Clitoris - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Clitoris_anatomy_labeled-en.svg" class="image">
 that is greatly enlarged to the point that they are categorized as intersexed. These people are identified immediately at birth as intersex because those with the condition have a sexual organ larger than a clitoris and smaller than a penis.
that is greatly enlarged to the point that they are categorized as intersexed. These people are identified immediately at birth as intersex because those with the condition have a sexual organ larger than a clitoris and smaller than a penis. - Simultaneous hermaphrodite (intersex) A simultaneous hermaphrodite (Homogamy - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Vista_Login_Manager_Cropped.svg" class="image">
 ) is a person that has both male and female sexual organs. This definition tends to be misleading since there have been very few human beings with fully developed male and female internal and external genitalia and female breasts. Normally one genitalia is more prominent than the other.
) is a person that has both male and female sexual organs. This definition tends to be misleading since there have been very few human beings with fully developed male and female internal and external genitalia and female breasts. Normally one genitalia is more prominent than the other.
 Some people who are intersex individuals, such as those with Klinefelter's syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Human_chromosomesXXY01.png" class="image">
Some people who are intersex individuals, such as those with Klinefelter's syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Human_chromosomesXXY01.png" class="image"> and Androgen insensitivity syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Androgen_receptor_3-d_model.jpg" class="image">
and Androgen insensitivity syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Androgen_receptor_3-d_model.jpg" class="image">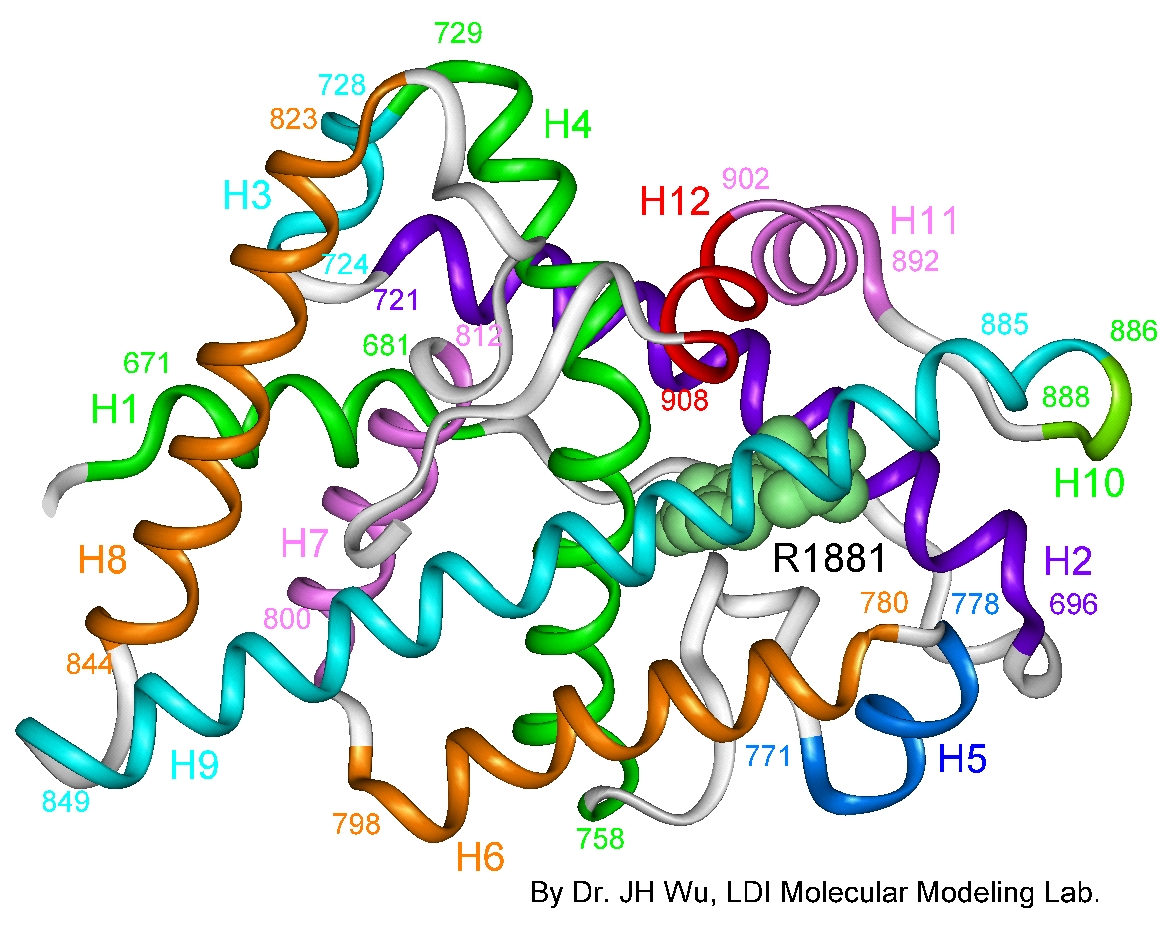 , appear completely female or male without realizing they are intersexed. An intersex person may express diversion from typical XX-female or XY-male chromosomes, for example a sex reversal of XY-female and XX-male.
, appear completely female or male without realizing they are intersexed. An intersex person may express diversion from typical XX-female or XY-male chromosomes, for example a sex reversal of XY-female and XX-male.
One of the most difficult experiences Reimer faced due to his increasingly unusual looks and behaviours was rejection from his peers. He became a pariah during his elementary school years. From as early as kindergarten, he was a target for bullying by both male and female. “As [I’d ]walk by, they’d start giggling. Not one, but almost the whole class. It’d be like that every day. The whole school would make fun of [me] about one thing or another.” In his early teens Reimer attended a technical high school. Right away his peers dubbed him Cave-woman and told him, “You’re a boy.” But it was his habit of urinating standing up that caused the greatest problem between Reimer and his schoolmates. The girls prevented him from using their bathroom. When he tried to use the boys’ room he was threatened with a knife. By December, he dropped out of school.
“When I say there was nothing feminine about David” Brian told John Colapinto, a writer for Rolling Stone magazine, “I mean there was nothing feminine. She walked like a guy. She talked about guy things, didn’t give a crap about cleaning house, getting married, wearing makeup…. We both wanted to play with guys, build forts and have snowball fights and play army.”
Along with struggling against emotional uncertainty about his life and his innate attraction to females, Reimer made no friends and was forcibly a loner. During puberty Reimer’s erroneous belief that he was a lesbian added to his emotional angst. The David Reimer case also serves to reinforce the scientific hypothesis that sexual orientation is not one of choice.
Eventually Reimer met a woman named Jane Fontaine, a single mother. They married and Reimer became both a husband and father. It was during this well-adjusted time in his life that Reimer discovered Dr. Money was still claiming that Reimer’s sex reassignment was highly successful. Money encouraged the medical and psychiatric communities to conduct the same procedures on children with genital deformities or ambiguous genitalia. Most likely it was due to two factors that Reimer chose to go public with his personal experience in an effort to contradict Money’s publications: he was secure within his marriage to a supportive spouse and he was determined to expose Money as a fraud. Reimer took part in public television and magazine interviews such as The Rolling Stone .Read David Reimer’s interview with John Colapinto.
 When released to the publicReimer’s story loosed an unexpected reaction. Intersex people born and reassigned after the publication of Money’s false protocols came forward with their stories. Among them was a San Francisco activist named Cheryl Chase/Brian Sullivan. When she was born Chase displayed ambiguous genitalia with a phallic structure of a size that, if she was female, could be an enlarged clitoris or if she was male, a micropenis. Her doctors assigned Chase as a boy and her parents named her Charlie. But 18 months later, her parents consulted another team of experts. Based partly on the fact that Chase had a fairly normal vagina, this team of doctors reassigned her as a girl. They amputated her phallus and her parents named her Cheryl. After the operation Cheryl refused to speak for 6 months. In 1995 Chase changed her name again to Bonnie Sullivan. In her mid-30′s Cheryl experienced a mental breakdown due to the reassignment of her gender. She made Hermaphrodites Speak! (1995), a 30 minute documentary film in which intersex people discuss the psychological impact of their conditions. Chase advocates a complex perspective of intersexuality, namely that gender difficulties cannot be eliminated by early genital surgery.
When released to the publicReimer’s story loosed an unexpected reaction. Intersex people born and reassigned after the publication of Money’s false protocols came forward with their stories. Among them was a San Francisco activist named Cheryl Chase/Brian Sullivan. When she was born Chase displayed ambiguous genitalia with a phallic structure of a size that, if she was female, could be an enlarged clitoris or if she was male, a micropenis. Her doctors assigned Chase as a boy and her parents named her Charlie. But 18 months later, her parents consulted another team of experts. Based partly on the fact that Chase had a fairly normal vagina, this team of doctors reassigned her as a girl. They amputated her phallus and her parents named her Cheryl. After the operation Cheryl refused to speak for 6 months. In 1995 Chase changed her name again to Bonnie Sullivan. In her mid-30′s Cheryl experienced a mental breakdown due to the reassignment of her gender. She made Hermaphrodites Speak! (1995), a 30 minute documentary film in which intersex people discuss the psychological impact of their conditions. Chase advocates a complex perspective of intersexuality, namely that gender difficulties cannot be eliminated by early genital surgery.
Years after Reimer’s public appearances, John Colapinto conducted a telephone interview with John Money, who refused to meet in person. His response to Calopinto`s observation that scientists and psychologists have disproven his book Man & Woman, Boy & Girl wherein he discussed the John-Joan experiment was, “It’s part of the antifeminist movement. They say masculinity and femininity are built into the genes, so women should get back to the mattress and the kitchen.” Money stood by his original summary of the Reimer case and dismissed Colapinto’s suggestion that he “misperceived” Reimer’s psychological condition. Colapinto reiterated that significant scientific evidence leaned towards the hypothesis that gender assignment was not as simple as reassigning gender, and asked Money if he was considering making some alternations to Man & Woman, Boy & Girl to which Money replied flatly, “I’ll be dead by then.” Suitably, an ambiguous answer from a man who spent most of his career misleading parents and children about ambiguous genitalia. Money also published a book still available for commercial purchase entitled Amazon.com: Gay, Straight, and In-Between: The Sexology of Erotic Orientation (978019506331 : John Money: Books@@AMEPARAM@@http://ecx.images-amazon.com/images/I/51Cxk1s3c3L.@@AMEPARAM@@51Cxk1s3c3L
: John Money: Books@@AMEPARAM@@http://ecx.images-amazon.com/images/I/51Cxk1s3c3L.@@AMEPARAM@@51Cxk1s3c3L
As with many family traumas Reimer’s sex reassignment deeply effected his whole family. “My parents feel very guilty, as if the whole thing was their fault,” Reimer told Colapinto. “But it wasn’t like that. They did what they did out of kindness, and love and desperation. When you’re desperate, you don’t necessarily do all the right things.” Reimer could not possibly have forseen the effect his public appearances would have on his brother Brian. Unable to accept Reimer’s openly candid description of his life, and still unable to accept that what was once his sister was now his brother, Brian committed suicide by drug overdose.
After Brian’s suicide Reimer experienced a series of unfortunate developments:his marriage disintegrated; he found himself unable to maintain stable employment; he experienced financial difficulty after making a poor investment; his anger at Dr. Money and the medical doctor responsible for his gender reassignment intensified; and his depression returned to haunt him. In May 2004 at the age of 38 Reimer committed suicide with a shotgun.
For several decades provinces in Canada have provided funding for people in need of SRS surgery. However the provinces differ in the amount of budgeting for intersex and reassignment surgery they offer, and also in its priority within the context of Canada`s medical community. Newfoundland, Quebec, Manitoba, Saskatchewan and B.C. currently cover SRS operations. Since 1969 SRS was covered in Ontario until funding was cut by
End Note: Not everyone who undergoes sex reassignment surgery lives a more satisfying life. Read Transsexual lottery winner regrets paying for gender reassignment.
Read Sex Change Regret
-
03-23-2011 #76Platinum Poster
- Join Date
- Mar 2006
- Location
- hollywood,calif
- Posts
- 7,071
 Re: tgirl lovers/admirers are gay yes??
Re: tgirl lovers/admirers are gay yes??
Born a Boy Raised a Girl The John/Joan/David Reimer Case and Sex Reassignment Surgery
Posted on November 5, 2010 by teacher
David Reimer - Wikipedia, the free encyclopedia, well known in medical and psychiatric circles specializing in gender Sex assignment - Wikipedia, the free encyclopedia, served as a ground-breaking study in regard to sexual orientation and sexual identity.
Reimer was born a boy with an identical (monozygotic) male twin. (Yes it is possible for a boy and a girl to be nearly identical and to have begun as monozygotic twins in the womb
if youre interested read my blog Seeing (almost) Double).
In 1966, a botched electrical Circumcision - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Circumcision_central_Asia2.jpg" class="image"> left David Reimer (then named Bruce) without a penis. A malfunction in the doctors equipment (electro-cautery needle) caused the needle to burn Reimers penis from tip to base. The Reimers were left with a dilemma: a son with no penis. They visited several medical experts who assured them that penile reconstruction would prove worthless. The Reimers were at a loss as to how to help David. One afternoon when the Reimers saw Dr. John Money, a so-called expert in sex reassignment, on television they contacted him and brought their son to see him. It would prove to be a tragic decision.
Money met with Brenda once a year throughout the following years to report on her progress. In spite of growing evidence that Brenda was not adjusting well to her gender reassignment, Money published papers to the contrary. In psychiatric circles to protect Reimers identity Money referred to Brenda as John/Joan . Moneys experiment became well-known in psychiatric communities worldwide and partly as a result of Moneys publications, a number of infants born with ambiguous genitalia underwent gender reassignment. However many psychologists were unconvinced about the John/Joan experiment. One of these was academic sexologist Milton Diamond - Wikipedia, the free encyclopedia, who, in a bold move against Money reported to the psychiatric community that Reimer never identified as female, and that he began living as a male from the age of 15.
Sexual reassignment in the Reimer case is not a gender identity disorder. He was born male unlike than intersex (Hermaphrodite - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Text_document_with_red_question_mark.svg" class="image">) individuals. Intersex - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Hermaphroditus,_from_a_Pompeiian_fresco,_c.18 00_(coloured_engraving)_by_French_School,_(19th_ce ntury).jpg" class="image"> is a term that usually defines discordance of the biological aspects of sexual gender. Traits related to the genitalia, such as internal organs, Gonad - Wikipedia, the free encyclopedia tissue, or Chromosome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Chromosome.svg" class="image"> that are more typical of the other sex, or incompletely Sexual differentiation - Wikipedia, the free encyclopedia define the intersex individual.Sub-types of hermaphroditism include:- Pseudohermaphroditism Typically a female has a Clitoris - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Clitoris_anatomy_labeled-en.svg" class="image"> that is greatly enlarged to the point that they are categorized as intersexed. These people are identified immediately at birth as intersex because those with the condition have a sexual organ larger than a clitoris and smaller than a penis.
- Simultaneous hermaphrodite (intersex) A simultaneous hermaphrodite (Homogamy - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Vista_Login_Manager_Cropped.svg" class="image">) is a person that has both male and female sexual organs. This definition tends to be misleading since there have been very few human beings with fully developed male and female internal and external genitalia and female breasts. Normally one genitalia is more prominent than the other.
Some people who are intersex individuals, such as those with Klinefelter's syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Human_chromosomesXXY01.png" class="image"> and Androgen insensitivity syndrome - Wikipedia, the free encyclopedia@@AMEPARAM@@/wiki/File:Androgen_receptor_3-d_model.jpg" class="image">, appear completely female or male without realizing they are intersexed. An intersex person may express diversion from typical XX-female or XY-male chromosomes, for example a sex reversal of XY-female and XX-male.
One of the most difficult experiences Reimer faced due to his increasingly unusual looks and behaviours was rejection from his peers. He became a pariah during his elementary school years. From as early as kindergarten, he was a target for bullying by both male and female. As [Id ]walk by, theyd start giggling. Not one, but almost the whole class. Itd be like that every day. The whole school would make fun of [me] about one thing or another. In his early teens Reimer attended a technical high school. Right away his peers dubbed him Cave-woman and told him, Youre a boy. But it was his habit of urinating standing up that caused the greatest problem between Reimer and his schoolmates. The girls prevented him from using their bathroom. When he tried to use the boys room he was threatened with a knife. By December, he dropped out of school.
When I say there was nothing feminine about David Brian told John Colapinto, a writer for Rolling Stone magazine, I mean there was nothing feminine. She walked like a guy. She talked about guy things, didnt give a crap about cleaning house, getting married, wearing makeup . We both wanted to play with guys, build forts and have snowball fights and play army.
Along with struggling against emotional uncertainty about his life and his innate attraction to females, Reimer made no friends and was forcibly a loner. During puberty Reimers erroneous belief that he was a lesbian added to his emotional angst. The David Reimer case also serves to reinforce the scientific hypothesis that sexual orientation is not one of choice.
Eventually Reimer met a woman named Jane Fontaine, a single mother. They married and Reimer became both a husband and father. It was during this well-adjusted time in his life that Reimer discovered Dr. Money was still claiming that Reimers sex reassignment was highly successful. Money encouraged the medical and psychiatric communities to conduct the same procedures on children with genital deformities or ambiguous genitalia. Most likely it was due to two factors that Reimer chose to go public with his personal experience in an effort to contradict Moneys publications: he was secure within his marriage to a supportive spouse and he was determined to expose Money as a fraud. Reimer took part in public television and magazine interviews such as The Rolling Stone .Read David Reimers interview with John Colapinto.
When released to the publicReimers story loosed an unexpected reaction. Intersex people born and reassigned after the publication of Moneys false protocols came forward with their stories. Among them was a San Francisco activist named Cheryl Chase/Brian Sullivan. When she was born Chase displayed ambiguous genitalia with a phallic structure of a size that, if she was female, could be an enlarged clitoris or if she was male, a micropenis. Her doctors assigned Chase as a boy and her parents named her Charlie. But 18 months later, her parents consulted another team of experts. Based partly on the fact that Chase had a fairly normal vagina, this team of doctors reassigned her as a girl. They amputated her phallus and her parents named her Cheryl. After the operation Cheryl refused to speak for 6 months. In 1995 Chase changed her name again to Bonnie Sullivan. In her mid-30′s Cheryl experienced a mental breakdown due to the reassignment of her gender. She made Hermaphrodites Speak! (1995), a 30 minute documentary film in which intersex people discuss the psychological impact of their conditions. Chase advocates a complex perspective of intersexuality, namely that gender difficulties cannot be eliminated by early genital surgery.
Years after Reimers public appearances, John Colapinto conducted a telephone interview with John Money, who refused to meet in person. His response to Calopinto`s observation that scientists and psychologists have disproven his book Man & Woman, Boy & Girl wherein he discussed the John-Joan experiment was, Its part of the antifeminist movement. They say masculinity and femininity are built into the genes, so women should get back to the mattress and the kitchen. Money stood by his original summary of the Reimer case and dismissed Colapintos suggestion that he misperceived Reimers psychological condition. Colapinto reiterated that significant scientific evidence leaned towards the hypothesis that gender assignment was not as simple as reassigning gender, and asked Money if he was considering making some alternations to Man & Woman, Boy & Girl to which Money replied flatly, Ill be dead by then. Suitably, an ambiguous answer from a man who spent most of his career misleading parents and children about ambiguous genitalia. Money also published a book still available for commercial purchase entitled Amazon.com: Gay, Straight, and In-Between: The Sexology of Erotic Orientation (978019506331: John Money: Books@@AMEPARAM@@http://ecx.images-amazon.com/images/I/51Cxk1s3c3L.@@AMEPARAM@@51Cxk1s3c3L
As with many family traumas Reimers sex reassignment deeply effected his whole family. My parents feel very guilty, as if the whole thing was their fault, Reimer told Colapinto. But it wasnt like that. They did what they did out of kindness, and love and desperation. When youre desperate, you dont necessarily do all the right things. Reimer could not possibly have forseen the effect his public appearances would have on his brother Brian. Unable to accept Reimers openly candid description of his life, and still unable to accept that what was once his sister was now his brother, Brian committed suicide by drug overdose.
After Brians suicide Reimer experienced a series of unfortunate developments:his marriage disintegrated; he found himself unable to maintain stable employment; he experienced financial difficulty after making a poor investment; his anger at Dr. Money and the medical doctor responsible for his gender reassignment intensified; and his depression returned to haunt him. In May 2004 at the age of 38 Reimer committed suicide with a shotgun.
For several decades provinces in Canada have provided funding for people in need of SRS surgery. However the provinces differ in the amount of budgeting for intersex and reassignment surgery they offer, and also in its priority within the context of Canada`s medical community. Newfoundland, Quebec, Manitoba, Saskatchewan and B.C. currently cover SRS operations. Since 1969 SRS was covered in Ontario until funding was cut by
End Note: Not everyone who undergoes sex reassignment surgery lives a more satisfying life. Read Transsexual lottery winner regrets paying for gender reassignment.
Read Sex Change Regret
-
03-23-2011 #77Platinum Poster
- Join Date
- Mar 2006
- Location
- hollywood,calif
- Posts
- 7,071
Re: tgirl lovers/admirers are gay yes??

http://caribbean.scielo.org/scielo.p...lng=en&nrm=iso
West Indian Medical Journal
Print ISSN 0043-3144
West Indian med. j. vol.55 no.6 Mona Jan. 2006
CASE REPORT
Hermaphroditism: cytogenetics, gonadal pathology and gender assignment a case report
Hermafroditismo: citogenética, patología gonadal y asignación de género
ND DuncanI; L GabayII; E WilliamsIII; SE DundasIV; N PlummerI; PA LeakeI
IDepartments of Surgery, Radiology, Anaesthesia and Intensive Care, The University of the West Indies, Kingston 7
IIDepartments of Obstetrics, Gynaecology and Child Health, The University of the West Indies, Kingston 7
IIIDepartments of Pathology, The University of the West Indies, Kingston 7
IVBustamante Hospital for Children, Arthur Wint Drive, Kingston 5, Jamaica
Correspondence
ABSTRACT
True hermaphroditism is a rare intersex disorder in which individuals possess both testicular and ovarian gonadal tissue. A case of true unilateral hermaphroditism presenting with ambiguous external genitalia, right scrotal testis and left pelvic ovotestis is herein outlined. Phallic, gonadal and genetic factors were considered before male gender was assigned. Gender assignment procedures have been questioned by intersex activists opposed to early genital surgery. Western societies have a binary perspective on gender and this leads to a stigma being placed on intersex cases. A multidisciplinary approach to this problem involving paediatric specialists in the field of endocrinology, surgery and psychiatry is necessary, along with educational programmes that promote tolerance in society to variations in gender.
RESUMEN
El verdadero hermafroditismo es un trastorno intersexual raro en el cual los individuos poseen tejido gonadal tanto testicular como ovárico. Aquí se describe en rasgos generales el caso de un verdadero hermafroditismo unilateral con genitales externos ambiguos, un testículo escrotal derecho y un ovotestículo pélvico izquierdo. Los factores fálicos, gonadales y genéticos fueron considerados antes de asignar el género masculino. Los procedimientos de asignación de género han sido cuestionados por activistas intersexuales que se oponen a la cirugía genital temprana. Las sociedades occidentales poseen una perspectiva binaria sobre el género y esto conduce a la estigmatización de los casos intersexuales. Se requiere un enfoque multidisciplinario de este problema, que involucre a pediatras especialistas en el campo de la endocrinología, la cirugía y la psiquiatría, simultáneamente con programas educacionales que promuevan la tolerancia de la sociedad frente a las variaciones de género.
INTRODUCTION
True hermaphrodites are unique individuals with both testicular and ovarian gonadal tissue (1). The term hermaphrodite is derived from the Greek mythological god Hermaphroditos, son of Hermes and Aphrodite, whose body, after being merged with the nymph Salmakis, assumed a more perfect form with both male and female attributes (2). True hermaphroditism falls within the spectrum of intersex disorders, manifesting discordance between genetic, gonadal and phenotypic sex. This spectrum includes masculinized genetic females (female pseudohermaphrodites), androgen deficient genetic males (male pseudohermaphrodites) and gonadal dysgenetics (2).
True hermaphrodites are categorized based on the type of gonadal asymmetry exhibited: true lateral hermaphrodites have one ovary and one testicle (27% of cases), bilateral hermaphrodites have both gonads as ovotestes (35% of cases) and unilateral hermaphrodites have one gonad as an ovotestis and the other as either an ovary or a testis (38% of cases) (3).
Those entrusted with the care of hermaphrodites know that gender assignment has become an increasingly controversial subject (4, 5). In this report, the management of a case of true unilateral hermaphroditism and a review of the literature on hermaphroditism as it relates to cytogenetics, gonadal pathology and gender assignment are presented.
CASE REPORT
A newborn with ambiguous genitalia was referred to the paediatric endocrinology service at the University Hospital of the West Indies, Kingston, Jamaica. Physical examination of the external genitalia revealed a 2.8 cm phallus (normal length 2.7 cm to 5.7 cm) with severe chordee and penoscrotal hypospadias (Fig. 1). The right hemiscrotum appeared normal and contained a normally descended gonad, but the left hemiscrotum was hypoplastic with ipsilateral cryptorchidism. Pelvic ultrasonography revealed a 2.6 cm x 1.4 cm x 1.7 cm homogenous mass lying posterior to the urinary bladder, with a 1.5 cm superior cystic component. These findings pointed to possible hermaphroditism.

Chromosomal analysis revealed a 46XX karyotype, despite the phallic structure and right scrotal gonad. No signal for the sry male-determining gene locus was detected. Groin exploration and laparotomy were performed to facilitate gonadal biopsies. The right scrotal gonad was biopsied via an inguinal approach. During this exploration, the left fallopian tube and attached gonad were noticed protruding through the right deep inguinal ring and therefore accessible through the same wound. Through the laparotomy incision, the left fallopian tube could be seen to be connected to a rudimentary left hemi-uterus. Pole to pole biopsies of both scrotal and prolapsed left adnexal gonads were performed.
Histological examination of the right scrotal gonad showed typical features of a testis with seminiferous tubules filled with Sertoli cells and spermatogonia, all lying within loose lamina propria containing Leydig cells (Fig. 2). The left adnexal gonad however was an ovotestis composed predominantly of primordial follicles in a spindle cell stroma with a solitary focus of testicular tissue at one pole (Fig. 3). A diagnosis of true unilateral hermaphroditism was made since both a right testis and a contralateral ovotestis were confirmed on histology.


The phallic length of 2.8 cm allowed for assignment of male sex of rearing in keeping with the parents wishes. A beta human chorionic gonadotropin stimulation test done after the gonadal biopsy showed a rise in serum testosterone level from 50 ng/dL to 235 ng/dL reflecting testicular function sufficient to sustain a male phenotype. The rudimentary uterus, left fallopian tube and left ovotestis were excised, in keeping with the recommended practice of removing contradictory gonads and internal genitalia (6). The penile hypospadias will be corrected by urethroplasty at age one year and arrangement will be made for follow-up by hospital social workers and a child psychiatrist.
DISCUSSION
The diagnosis of true hermaphroditism requires histological proof of both testicular and ovarian tissue occurring in the same individual (1, 6, 7). Ovotestes are the gonads most commonly detected in hermaphrodites, with ovaries and testes following in order of prevalence (.
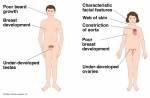
The appearance of the external genitalia ranges from normal male to normal female but many have ambiguous genitalia, manifesting phallic chordee, hypospadias and cryptorchidism (6, 7). The non-specific appearance of external genitalia results in many cases of hermaphroditism being missed at birth, only to come to light at puberty when amenorrhoea presents in patients raised as girls or breast development causes alarm in patients raised as boys (3, 6). A high index of suspicion is necessary to reduce the frequency of late diagnosis. To this end, patients with hypospadias and cryptorchidism should be subjected to early laparotomy and biopsy of gonads (6).
The distribution of ovarian and testicular tissue within ovotestes varies from case to case with one moiety predominating and the other assuming a polar or hilar distribution (. Gonadal biopsies should therefore be performed from pole to pole extending deep into the hilum of the gonad (1, .
Having determined hermaphroditism, assignment of an appropriate gender becomes urgent. Traditionally, a multidisciplinary team of healthcare professionals comprised of paediatrician, paediatric endocrinologist, paediatric surgeon and paediatric psychiatrist meet with parents and assign a sex of rearing based on genital, gonadal and genetic factors (5). Phallic size and its potential to develop into a sexually functional organ have long been held to be the most important factors in the choice of male sex of rearing (8–10). Female sex of rearing is the likely choice when phallic length is below 1.5 cm because an adequate and functional vagina can be more reliably constructed in that setting than a functional penis (.
Gonadal factors are also important in the choice of sex of rearing. Whatever decision is made, there must be adequate functioning gonadal tissue present to sustain the sex of rearing, and gonads producing contradictory hormones should be excised (6). This guided the decision to excise the left ovotestis while preserving the right testis. Malignant gonadal tumours occur in 1.91% of true hermaphrodites, most commonly arising in patients with a 46XY karyotype and in dysgenetic or undescended testes (1, 8, 10). Though the right testis was shown to be histologically normal and descended, the decision to preserve the gonad in this patient mandates long-term follow-up and screening for testicular neoplasms.
A patients genetic sex, as determined by karyotype studies, is not always the appropriate choice for sex of rearing in hermaphrodites. The 46XX karyotype occurs in 60% to 70% of hermaphrodites (1, 2,, while 46XX/46XY mosaicism and 46XY genetic males are seen less commonly. Although the Y chromosome predisposes to a male phenotype in 46XY karyotypes, a 46XX karyotype does not necessarily promote a female sex of rearing. This is because the testis-inducing sry locus, normally located on the short arm of the Y chromosome, can sometimes become transferred to an X chromosome during meiotic division of a primary spermatocyte (1,6). Thus 46XX patients may have not only a testis, but also normal testosterone production. Despite evident testosterone production, the sry gene locus was not found in this case, suggesting that subtler gene translocations may suffice to cause development of male characteristics. Mosaic karyotypes such as 46XX/46XY are thought to result from chimerism, possibly from double fertilization (involving two spermatocytes-one X and one Y) of either a binucleate ovum or of an ovum and its polar body.
The process by which healthcare professionals and parents have consultations to assign gender to intersex cases is called the paternalistic approach (11). This approach is based on the concept that children are gender neutral at birth and can be made to assume male or female characteristics through a combination of psychosocial rearing and "nor-malizing genital surgery" in infancy (12). Patients are generally not told about their intersex status during childhood to avoid mental trauma and psychosexual conflicts (13).
Vehement opposition to the paternalistic approach has come from intersex activists led by The Intersex Society of North America (ISNA), a group constituted largely of inter-sex adult patients who have become disappointed with their assigned gender (12–14). These intersex activists have challenged many of the time-honoured practices of gender practitioners, including early genital surgery, which they say damages sexual sensation and disrupts intimacy in adult life (14). Applying standard ethical principles, they propose that genital surgery be delayed until when patients are able to give informed consent (13, 14). They also plead for patients to receive age appropriate medical disclosure, aggressive mental counselling and peer support therapy (14, 15). They dismiss as flawed, emphasis on phallic length and functionality in the determination of male sex of rearing (12). The merit of positions adopted by these intersex activists has been affirmed by the British Association of Paediatric Surgeons Working Party on the Surgical Management of Children born with Ambiguous Genitalia. This group, while recognizing standard protocols on gender assignment, proposed that parents be allowed to consider the option of non-operative management with psychosocial support before consenting to early genital surgery (15).
Newer concepts on the genesis of gender, focus on gender as the product of genetic and endocrine influences on the brain during intrauterine life (13, 16, 17). Workers have come to view gender as an innate quality with three aspects to it: gender role (which relates to dress, speech and gestures), gender identity (the gender of ones self image) and psychosexual preference (homosexuality, heterosexuality or bisexuality) (13) and variation occurs on each level leading to many possibilities (11, 13). Because western societies have a binary perspective on sex and gender (13), bizarre labels are placed on anyone not viewed to be a normal male or normal female. This leads to stigmatization of intersex patients and their families (11). While it is clear that a multidisciplinary approach to clinical care is best for intersex cases, educational programmes that increase tolerance to variations in gender are also necessary.
REFERENCES
1. Donahoe PK, Crawford JD, Hendren WH. True hermaphroditism: a clinical description and a proposed function for the long arm of the Y chromosome. J Pediatr Surg 1978; 13: 293–301. [ Links ] 2. Fallat ME. Ambiguous genitalia and intersex anomalies. In: Ziegler MM, Azizkhan RG, Weber TR. ed. Operative Paediatric Surgery. New York: McGraw-Hill Companies; 2003: 839–61.
3. Wiersma R. Management of the African child with true herma-phroditism. J Pediatr Surg 2001; 36: 397–9.
4. Nihoul-Fékété C. The Isabel Forshall Lecture. Surgical management of the intersex patient: an overview in 2003. J Pediatr Surg 2004; 39: 144–5.
5. Reiner WG. Sex assignment in the neonate with intersex or inadequate genitalia Arch Pediatr Adolesc Med 1997; 151: 1044–5.
6. Olsson CA, Tessier PA, Brown ML, Austen G Jr. True hermaphroditism. J Urol 1971; 105: 586–90.
7. Luks FI, Hansbrough F, Klotz DH, Kottmeier PK, Tolete-Velcek F. Early gender assignment in true hermaphroditism. J Pediatr Surg 1988; 23: 1122–6.
8. van Niekerk WA. True hermaphroditism. An analytical review with a report of 3 new cases. Am J Obstet Gynecol 1976; 126: 890–907.
9. Burstein S, Grumbach MM, Kaplan SL. Early determination of androgen-responsiveness is important in the management of microphallus. Lancet 1979; 2: 983 – 6.
10. Evaluation of the newborn with developmental anomalies of the external genitalia. American Academy of Pediatrics, Committee on Genetics. Pediatrics 2000; 106: 138–42.
11. Blizzard RM. Intersex issues: A series of continuing Conundrums. Pediatrics 2002; 110: 616–21.
12. Dreger AD. "Ambiguous sex" – or ambivalent medicine? Ethical issues in the medical treatment of intersexuality. Hastings Cent Rep 1998; 28: 24–35.
13. Kipnis K, Diamond M. Paediatric ethics and the surgical assignment of sex. J Clin Ethics 1998; 9: 398–410.
14. Chase C. What is the agenda of the intersex patient advocacy movement? Endocrinologist 2003; 13: 240–2.
15. British Association of Paediatric Surgeons working party statement on the surgical management of children born with ambiguous genitalia July 2001.
16. Phornphutkul C, Fausto-Sterling A, Gruppuso PA. Gender self-reassignment in an XY adolescent female born with ambiguous genitalia. Pediatrics 2000; 106: 135 – 7.
17. Diamond M, Sigmundson HK. Management of intersexuality guidelines for dealing with persons with ambiguous genitalia. Arch Pediatrolesc Med 1997; 151: 1046 – 50.
 Correspondence:
Correspondence:
Dr ND Duncan
Department of Surgery, Radiology, Anaesthesia and Intensive Care, The University of the West Indies
Kingston 7, Jamaica.
The University of the West Indies
Kingston, 7
Mona - Jamaica
Tel.: (876) 927-1214
Fax.: (876) 927-1846
-
03-24-2011 #78Junior Poster
- Join Date
- Jan 2008
- Location
- ohio
- Posts
- 251
Re: tgirl lovers/admirers are gay yes??
that was one chart to many for me
-
03-24-2011 #79Gold Poster
- Join Date
- Mar 2011
- Location
- Parts Unknown
- Posts
- 5,236
Re: tgirl lovers/admirers are gay yes??
Damn! This thread turned into a course in biology!
 So when is the essay due from the info we're learning about on here? Can we use notes on the test?
So when is the essay due from the info we're learning about on here? Can we use notes on the test?
-
03-24-2011 #80Platinum Poster

- Join Date
- Feb 2011
- Location
- York UK
- Posts
- 12,089
Re: tgirl lovers/admirers are gay yes??
Maybe, but it's kept the OP quiet for a while.

 Reply With Quote
Reply With Quote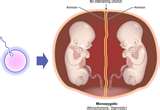



Similar Threads
-
Tgirl admirers: Webcam chat, personals, and video sharing
By TSGina in forum The Buy/Sell/Trade BoardReplies: 1Last Post: 05-22-2011, 04:01 PM -
Girls Only: Admirers, Chasers or Lovers
By evilernie in forum General DiscussionReplies: 12Last Post: 09-30-2010, 06:31 PM -
How many TGirl admirers are married?
By mreef in forum General DiscussionReplies: 13Last Post: 11-04-2005, 09:01 PM